Introduction
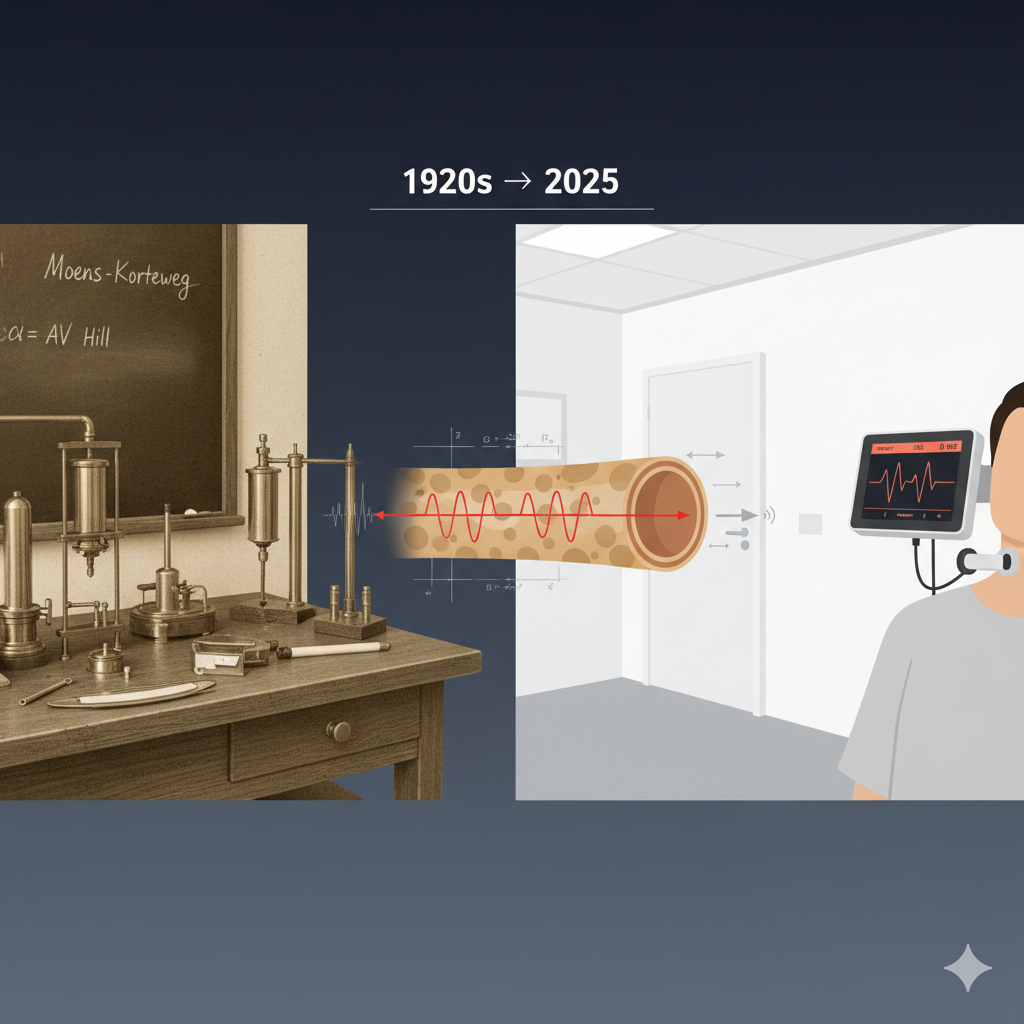
From AV Hill’s 1920s physiology lab to today’s cardiovascular clinics, one measurement connects them: pulse wave velocity. This seemingly simple metric—how fast a pressure wave travels through your arteries—bridges a century of scientific evolution.[1] What began as pure physics has become one of the most powerful predictors of cardiovascular risk we possess.
Understanding pulse wave velocity (PWV) means understanding arterial stiffness, the silent process of vascular aging that precedes heart attacks and strokes by decades.[2] As arteries lose elasticity through arteriosclerosis and hypertension, pressure waves race faster through rigid vessels. This acceleration tells a story about cardiovascular disease long before symptoms emerge.
PWV transforms abstract arterial mechanics into quantifiable cardiovascular risk assessment.[3] It’s a window into hemodynamic parameters that blood pressure alone cannot reveal. The measurement captures the mechanical consequences of endothelial dysfunction, arterial compliance loss, and structural changes in vessel walls—all critical elements of vascular aging.
| Objective | Outcome |
|---|---|
| Understand PWV physics | Grasp the Moens-Korteweg equation and elastic modulus relationship |
| Trace historical evolution | Connect AV Hill’s foundational work to modern applications |
| Explore clinical applications | Learn why PWV predicts cardiovascular events |
| Review measurement methods | Understand non-invasive assessment techniques like tonometry |
The Physics Behind the Pulse: From Moens-Korteweg to Modern Medicine
The physics of pulse wave velocity rests on a remarkably elegant principle: waves travel faster through stiffer materials. When your heart contracts, it generates a pressure wave that propagates through the arterial tree. The speed of this wave depends entirely on the mechanical properties of vessel walls.[4]
Enter the Moens-Korteweg equation, derived in the 1870s-1890s: PWV = √(Eh/2ρr), where E represents the elastic modulus of the arterial wall, h is wall thickness, ρ is blood density, and r is vessel radius.[5] This equation reveals that PWV increases with wall stiffness and decreases with vessel diameter. AV Hill, who won the Nobel Prize in 1922 for his work on muscle physiology, made crucial contributions to understanding how these vascular mechanics relate to cardiovascular function.[6]
The relationship between arterial compliance and wave speed explains why healthy, elastic arteries slow pulse waves to 5-7 m/s, while stiffened vessels in older adults or those with hypertension can exceed 15 m/s. These hemodynamic parameters reflect fundamental changes in arterial wall structure—collagen accumulation, elastin fragmentation, and calcification that characterize arteriosclerosis.
Key Point: Stiffer arteries = faster pulse waves = higher cardiovascular risk
Measuring What Matters: PWV Assessment Methods
| Method | Measurement Site | Gold Standard | Clinical Use |
|---|---|---|---|
| Carotid-Femoral PWV | Carotid to femoral artery | Yes | Aortic stiffness, cardiovascular risk stratification |
| Brachial-Ankle PWV | Arm to ankle | No | Screening, peripheral vascular assessment |
| Aortic PWV (MRI) | Ascending to descending aorta | Reference standard | Research, detailed vascular characterization |
| Tonometry-Based | Radial or carotid artery | No | Central blood pressure, wave reflection analysis |
The evolution from invasive catheter-based measurements to non-invasive assessment represents a triumph of biomedical engineering. Early PWV studies required arterial punctures and pressure transducers inserted directly into vessels. Modern approaches use surface tonometry—gentle pressure sensors placed over accessible arteries like the carotid and femoral.[7]
Carotid-femoral PWV has emerged as the gold standard because it captures aortic stiffness, and the aorta bears the brunt of pressure wave forces with each heartbeat.[8] The measurement is straightforward: record the pulse wave at the carotid artery, then at the femoral artery. The time delay between arrivals, divided by the distance traveled, yields PWV. Values below 10 m/s are generally considered normal in adults, while values exceeding 12-13 m/s indicate substantially increased cardiovascular risk.
Modern devices have streamlined the process. Automated systems measure PWV in minutes, calculating not just velocity but also central blood pressure and wave reflection patterns. This comprehensive vascular phenotyping provides insights impossible to glean from brachial blood pressure cuffs alone.
Key Point: Gold standard—carotid-femoral PWV >10 m/s indicates increased cardiovascular risk
Why PWV Matters: Predicting Cardiovascular Events
| PWV Range (m/s) | Risk Category | Clinical Interpretation |
|---|---|---|
| <7 m/s | Low | Healthy arterial compliance, typical in younger adults |
| 7-10 m/s | Moderate | Age-related stiffening, monitor cardiovascular risk factors |
| 10-13 m/s | Elevated | Increased CV risk, consider intervention |
| >13 m/s | High | Substantially increased risk, aggressive management recommended |
PWV’s clinical power lies in its ability to predict cardiovascular events independently of traditional risk factors like blood pressure, cholesterol, and diabetes.[9] Meta-analyses consistently show that each 1 m/s increase in aortic PWV corresponds to approximately 15% increased risk of cardiovascular events and all-cause mortality. This relationship persists even after adjusting for conventional risk factors, suggesting PWV captures pathophysiology that other measurements miss.
The mechanism makes biological sense. Arterial stiffness isn’t just a marker—it’s a mediator of cardiovascular disease. Stiff arteries increase cardiac workload, reduce coronary perfusion, and generate excessive pressure pulsatility that damages the microvasculature of the brain and kidneys.[10] PWV measurement quantifies these destructive hemodynamic forces before they manifest as clinical events.
Consider hypertension, where PWV serves as a superior hypertension biomarker compared to brachial blood pressure alone. Two individuals with identical arm pressures can have vastly different aortic stiffness, and the person with higher PWV faces greater cardiovascular risk. This explains why some treated hypertensive patients continue experiencing events despite “controlled” blood pressure—their arterial walls remain pathologically stiff.
Key Point: PWV adds predictive value beyond blood pressure alone—it captures arterial wall changes decades before events
The Takeaway
Pulse wave velocity connects AV Hill’s foundational physics from a century ago to modern cardiovascular risk stratification in today’s clinics. What emerged from understanding elastic properties of biological tissues has evolved into a powerful clinical tool that predicts heart attacks and strokes years before they occur. Understanding the mechanics of PWV reveals why arterial stiffness matters profoundly for cardiovascular health—it’s not just a consequence of aging and disease, but an active contributor to cardiovascular events that can be measured, monitored, and potentially modified.
“Pulse wave velocity transforms the invisible mechanical properties of our arteries into a measurable predictor of cardiovascular futures”
— Key finding from cardiovascular outcome meta-analyses
References
- Laurent S, Cockcroft J, Van Bortel L, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27(21):2588-2605. doi:10.1093/eurheartj/ehl254 PMID: 17000623
- Safar ME, Levy BI, Struijker-Boudier H. Current perspectives on arterial stiffness and pulse pressure in hypertension and cardiovascular diseases. Circulation. 2003;107(22):2864-2869. doi:10.1161/01.CIR.0000069826.36125.B4 PMID: 12796414
- Townsend RR, Wilkinson IB, Schiffrin EL, et al. Recommendations for improving and standardizing vascular research on arterial stiffness. Hypertension. 2015;66(3):698-722. doi:10.1161/HYP.0000000000000033 PMID: 26160955
- Bramwell JC, Hill AV. The velocity of the pulse wave in man. Proc R Soc Lond B Biol Sci. 1922;93(652):298-306. doi:10.1098/rspb.1922.0022
- Nichols WW, O’Rourke MF, Vlachopoulos C. McDonald’s Blood Flow in Arteries: Theoretical, Experimental and Clinical Principles. 6th ed. CRC Press; 2011.
- Hill AV. The revolution in muscle physiology. Physiol Rev. 1932;12(1):56-67. doi:10.1152/physrev.1932.12.1.56
- Van Bortel LM, Laurent S, Boutouyrie P, et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J Hypertens. 2012;30(3):445-448. doi:10.1097/HJH.0b013e32834fa8b0 PMID: 22278144
- Reference Values for Arterial Stiffness’ Collaboration. Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors. Eur Heart J. 2010;31(19):2338-2350. doi:10.1093/eurheartj/ehq165 PMID: 20530030
- Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness. J Am Coll Cardiol. 2010;55(13):1318-1327. doi:10.1016/j.jacc.2009.10.061 PMID: 20338492
- Mitchell GF, Hwang SJ, Vasan RS, et al. Arterial stiffness and cardiovascular events: the Framingham Heart Study. Circulation. 2010;121(4):505-511. doi:10.1161/CIRCULATIONAHA.109.886655 PMID: 20083680
Useful Resources
- European Society of Cardiology Guidelines on Arterial Stiffness – Comprehensive clinical recommendations for PWV assessment and interpretation in cardiovascular risk management
- NIH National Heart, Lung, and Blood Institute: Arterial Stiffness Overview – Patient-friendly explanation of vascular aging and measurement techniques
- American Heart Association: Understanding Vascular Assessment – Educational materials on pulse wave analysis and cardiovascular health
- AV Hill Nobel Prize Lecture Archive – Historical perspective on the physiological foundations of cardiovascular mechanics
Frequently Asked Questions
What’s a normal pulse wave velocity?
Normal PWV varies by age, but generally values below 10 m/s are considered healthy for adults. Younger individuals typically measure 5-7 m/s, while values increase with age. The European Society of Cardiology guidelines provide age-specific reference ranges, and this reference values study offers detailed normative data across populations.
How is pulse wave velocity measured?
The gold standard method is carotid-femoral PWV using applanation tonometry—gentle pressure sensors placed over arteries to detect pulse waves. The measurement takes about 10-15 minutes and is completely non-invasive. Watch this demonstration video or read the AHA scientific statement on measurement standardization for technical details.
Can pulse wave velocity be improved?
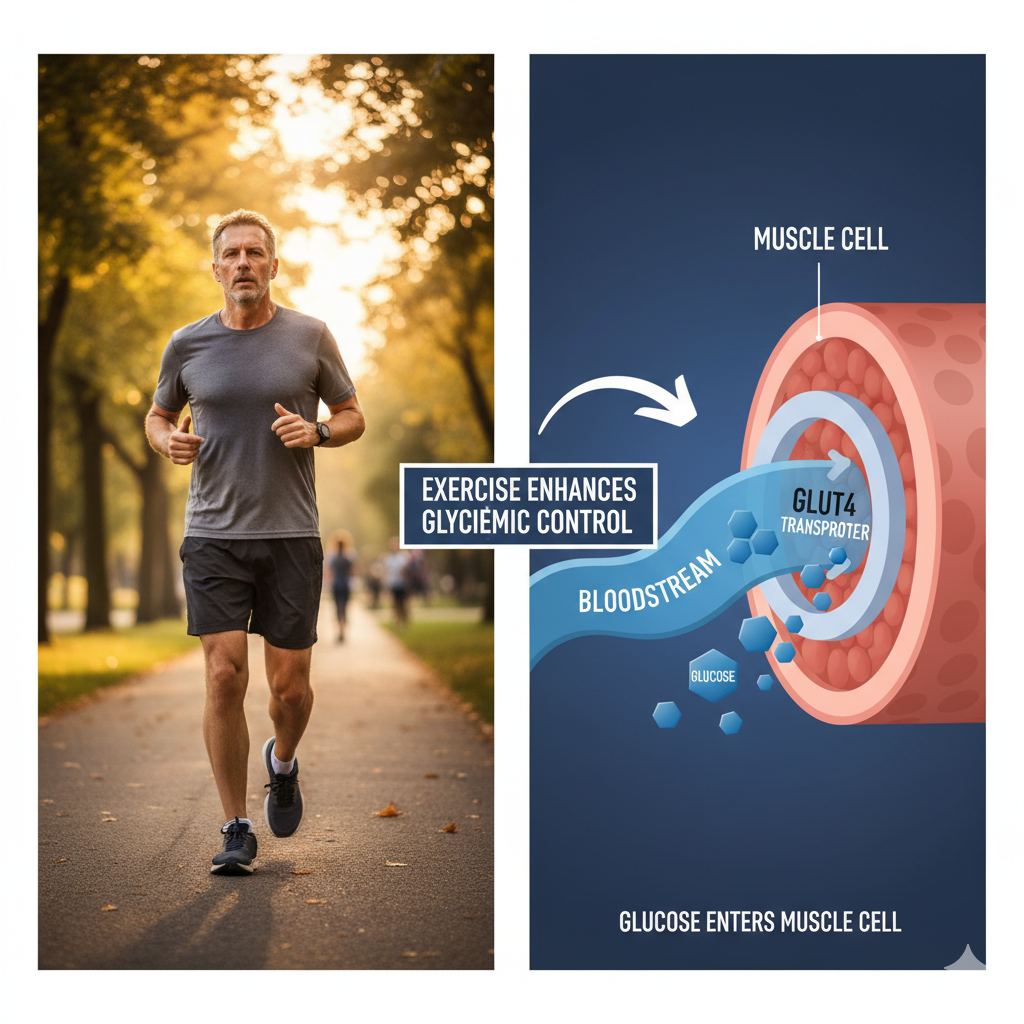
Yes, arterial stiffness can be reduced through lifestyle interventions. Regular aerobic exercise, particularly endurance training, consistently reduces PWV by 1-2 m/s. Blood pressure control with certain antihypertensive medications also improves arterial compliance. This review on lifestyle interventions and this study on exercise effects provide evidence-based recommendations.
PWV versus blood pressure—which matters more?
Both matter, but they measure different things. Blood pressure captures instantaneous force, while PWV reflects chronic arterial wall damage. Meta-analyses show PWV predicts cardiovascular events independently of blood pressure, suggesting it adds complementary information. This landmark meta-analysis demonstrates PWV’s independent predictive value beyond traditional risk factors.
Is PWV testing covered by insurance?
Coverage varies by country and insurance plan. In the United States, PWV measurement is not routinely reimbursed as a screening test, though it may be covered in research settings or for specific high-risk patients. European guidelines increasingly recognize PWV for cardiovascular risk stratification. Check the Medicare coverage database or consult your insurance provider for specific coverage policies.
Future Blog Topics
| Upcoming Article | Coming Soon | Why It Matters |
|---|---|---|
| Reversing Arterial Stiffness: Evidence-Based Interventions | Next week | Learn which exercise protocols, dietary patterns, and medications actually reduce PWV based on clinical trial evidence |
| Central vs Peripheral Blood Pressure: Why Your Aorta Tells a Different Story | 2 weeks | Discover why arm cuff pressure misses critical information about wave reflection and central aortic stress |
| The Endothelium Connection: How Vascular Function Affects Stiffness | 3 weeks | Explore the bidirectional relationship between endothelial dysfunction, nitric oxide, and arterial mechanical properties |

Leave a Reply