Introduction
Every year, approximately 795,000 people in the United States experience a stroke, and recurrent stroke occurs in approximately 25% of patients within the first year, with 5-year cumulative risk reaching 30-40%.[1] Yet despite clear clinical guidelines for post-stroke behavior change, fewer than 30% of stroke survivors achieve recommended physical activity levels.[2] This behavior change gap represents not just a clinical challenge, but a critical policy opportunity.
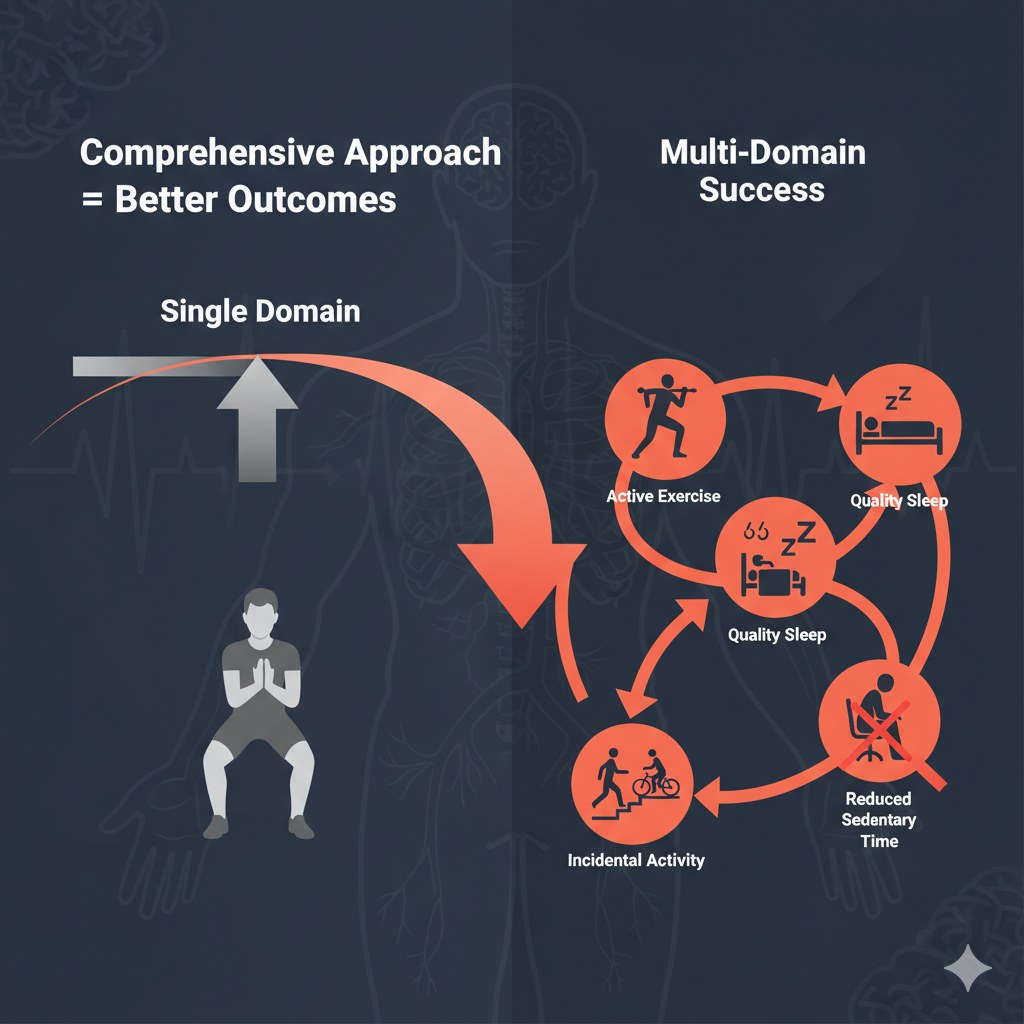
Understanding why some stroke and TIA (transient ischemic attack, or “mini-stroke”) survivors successfully modify their lifestyles while others struggle requires examining the frameworks we use to guide intervention design. Traditional approaches often focus on single behaviors—typically exercise—but emerging evidence reveals a more complex reality. The interconnected nature of physical activity, sedentary behavior, sleep quality, and incidental movement demands a more sophisticated approach.
Comparing behavior change models reveals that successful stroke recovery programs must address multiple behavioral domains—exercise, incidental activity, sedentary time, and sleep—rather than focusing on single interventions.[3] For policymakers and healthcare leaders, this insight transforms how we design, fund, and implement stroke recovery initiatives.
| Learning Objective | Expected Outcome |
|---|---|
| Understand key behavior change models and their application to stroke recovery | Identify which theoretical frameworks best match your program goals |
| Recognize why multi-domain interventions outperform single-behavior approaches | Design comprehensive programs addressing the full 24-hour movement spectrum |
| Learn cost-effective implementation strategies for holistic stroke recovery programs | Make evidence-based policy decisions that improve outcomes while managing resources |
Understanding Behavior Change Models
When designing stroke recovery programs, the theoretical framework matters. Three dominant models shape how we approach behavior change, and each offers valuable—but incomplete—insights for post-stroke intervention. Understanding these frameworks helps policymakers make informed decisions about program design and resource allocation.
The Health Belief Model focuses on individual perceptions of stroke risk and recovery benefits. This framework predicts that survivors who perceive high risk of recurrent stroke and believe behavior change will reduce that risk are most likely to adopt healthier lifestyles.[4] While useful for understanding motivation, this model often overlooks the social and environmental barriers that prevent action even when motivation is high. For example, a stroke survivor may understand the importance of daily exercise but lack access to accessible facilities or transportation.
The Theory of Planned Behavior adds crucial social dimensions by considering how family expectations, healthcare provider recommendations, and community norms influence behavior intentions. Research shows that stroke survivors with strong social support networks achieve better adherence to physical activity recommendations.[5] Furthermore, this model emphasizes perceived behavioral control—the survivor’s confidence in their ability to change. Integrated interventions based on combined Health Belief Model and Theory of Planned Behavior principles have shown improved self-management ability and quality of life in stroke patients.[6]
Social Cognitive Theory, developed by Albert Bandura, takes the most comprehensive view by recognizing that behavior, personal factors, and environment interact reciprocally. This model emphasizes self-efficacy—the belief in one’s capability to execute behaviors—as central to behavior change.[7] Importantly, Social Cognitive Theory acknowledges that changing the environment can be as important as changing individual attitudes. For stroke survivors, this might mean modifying home layouts to facilitate movement or building partnerships with community organizations to provide accessible exercise options.
Key Point: Each behavior change model addresses different barriers to post-stroke lifestyle modification, but none fully captures the complexity alone. Effective programs often integrate elements from multiple frameworks.
The Multi-Domain Imperative
| Intervention Approach | Components Targeted | Outcome Evidence |
|---|---|---|
| Single-Domain (Exercise Only) | Moderate-vigorous physical activity (MVPA) | Limited impact on recurrence risk; does not address sedentary time or sleep |
| Multi-Domain (Comprehensive) | Exercise + sedentary behavior reduction + sleep optimization + incidental activity | Improved function, mental health, reduced recurrence risk; addresses full 24-hour spectrum |
| PA + Sedentary Behavior | Physical activity targets + sitting time reduction | Promising but requires both behaviors simultaneously; less than 30% of survivors meet PA guidelines alone |
Evidence increasingly shows that post-stroke recovery requires addressing the entire 24-hour movement spectrum, not isolated behaviors. First, we must understand a critical distinction: physical inactivity (not meeting recommended activity levels) differs from sedentary behavior (sitting or reclining with energy expenditure ≤1.5 METs).[8] A stroke survivor can be both highly sedentary and physically active on the same day—for example, meeting exercise guidelines with a 30-minute walk but spending 10+ hours sitting.
Less than 30% of stroke survivors achieve recommended physical activity levels, and high levels of sedentary behavior are consistently reported.[9] Multi-faceted behavioral interventions targeting both physical activity and sedentary behavior throughout the rehabilitation pathway show promise for improving outcomes. These programs use behavior change techniques like problem-solving, goal-setting, and self-monitoring, tailored to individual needs with training for healthcare professionals delivering the intervention.[9]
Sleep represents another critical—yet often overlooked—component of stroke recovery. Sleep disorders are frequent after stroke, with up to 60% of patients showing abnormal breathing patterns approximately three months post-stroke.[10] People with stroke and sleep disorders have significantly greater functional limitations, with Barthel Index scores averaging 10.2 points lower than those without sleep disorders.[11] Sleep appears to function as a “plasticity state” that consolidates motor learning from rehabilitation exercises and promotes neuroplasticity essential for recovery.[12]
Key Point: Post-stroke recovery requires addressing the full 24-hour movement spectrum: exercise, incidental activity, sedentary time reduction, and sleep optimization. Targeting only exercise leaves most of the day unaddressed.
Policy Implications and Cost-Effectiveness
| Program Type | Cost Metrics | Cost-Effectiveness Evidence |
|---|---|---|
| Comprehensive Stroke Services | £5,228 (≈$6,900 USD) per QALY | 9.8% absolute reduction in death/dependency; highly cost-effective versus usual care |
| COMPASS Transitional Care | $74,975 annual implementation cost | Could lower net costs if preventing ≥6 readmissions/year (avg. readmission: $14,200) |
| Enhanced Home-Based Care | Nurse-led with multidisciplinary support | Reduced readmissions, improved QALYs, cost-effective with organized rehabilitation |
The economic argument for comprehensive, multi-domain stroke recovery programs is compelling. Full implementation of comprehensive stroke services was associated with a 9.8% absolute reduction in risk of death or dependency, with an incremental cost-effectiveness ratio of approximately $6,900 USD per quality-adjusted life year (QALY) gained.[13] This falls well below commonly cited willingness-to-pay thresholds, making comprehensive stroke care highly cost-effective compared to standard care.
Transitional care models like COMPASS (Comprehensive Post-Acute Stroke Services) demonstrate feasible implementation costs. With an average annual cost of approximately $75,000 for implementation, COMPASS could lower net healthcare costs if the model prevents just six hospital readmissions per year—given that the average 30-day readmission for ischemic stroke costs around $14,200.[14] Results from the COMPASS trial suggest that comprehensive transitional care significantly improves patient outcomes, particularly when implemented with fidelity across multiple sites.
What makes these programs cost-effective? Several factors contribute: reduced recurrent stroke rates (with each recurrence costing an average of $17,121 in hospital costs plus $34,639 in disability costs annually), improved functional independence reducing long-term care needs, decreased depression and improved quality of life, and prevention of complications through better self-management. Enhanced post-discharge home-based care programs delivered by nurse case managers supported by interdisciplinary teams have demonstrated cost-effectiveness through reduced readmissions, shorter hospital stays, and improved health-related quality of life.[15]
For policymakers, the evidence is clear: comprehensive programs addressing multiple behavioral domains offer superior return on investment compared to fragmented, single-behavior interventions. The key is ensuring programs are evidence-based, implemented with fidelity, and include adequate training and support for healthcare professionals. Short-term rehabilitation pathways followed by community clinic support have also proven cost-effective from both individual and healthcare service perspectives.[16]
Key Point: Holistic behavior change programs show superior cost-effectiveness through reduced recurrent stroke rates, improved functional independence, and decreased long-term care costs. Investing in comprehensive programs yields measurable returns.
Takeaway
Understanding the evidence behind different behavior change models enables leaders to design more effective, cost-efficient stroke recovery policies that address the whole person, not just isolated behaviors. By moving beyond single-domain interventions to comprehensive programs that integrate behavior change theory with practical support for exercise, sedentary behavior reduction, sleep optimization, and incidental activity throughout the day, policymakers can significantly improve outcomes while demonstrating measurable return on investment through reduced recurrence rates and enhanced functional independence.
“Comprehensive stroke care that addresses the full continuum of prevention and recovery represents not just good medicine, but sound fiscal policy.”
— European Brain Council Value of Treatment Initiative
References
- Ovbiagele B, Saver JL, Fredieu A, et al. Improving adherence to secondary stroke prevention strategies through motivational interviewing. Stroke. 2004;35(12):2867-2872.
- Moore SA, Hallsworth K, Jakovljevic DG, et al. How should long-term free-living physical activity be targeted after stroke? A systematic review and narrative synthesis. Int J Behav Nutr Phys Act. 2018;15(1):100.
- Aguiar LT, Martins JC, Lara EM, et al. Influence of interventions on daily physical activity and sedentary behavior after stroke: A systematic review. Am J Phys Med Rehabil. 2019;98(11):1031-1038.
- Jones CL, Jensen JD, Scherr CL, et al. The Health Belief Model as an explanatory framework in communication research: exploring parallel, serial, and moderated mediation. Health Commun. 2015;30(6):566-576.
- Lawrence M, Celestino Junior FT, Matozinho HH, et al. Predictors of adherence to lifestyle recommendations in stroke secondary prevention. Int J Environ Res Public Health. 2021;18(9):4666.
- Zhang YY, Zhou LL, Jiang WJ, et al. Effects of self-management intervention programs based on the health belief model and planned behavior theory on self-management behavior and quality of life in middle-aged stroke patients. Evid Based Complement Alternat Med. 2021;2021:5185933.
- Bandura A. Health promotion by social cognitive means. Health Educ Behav. 2004;31(2):143-164.
- Tremblay MS, Aubert S, Barnes JD, et al. Sedentary behavior research network (SBRN) – terminology consensus project process and outcome. Int J Behav Nutr Phys Act. 2017;14(1):75.
- Moore SA, Avery L, Flynn D, et al. Using intervention mapping to develop and facilitate implementation of a multifaceted behavioural intervention targeting physical activity and sedentary behaviour in stroke survivors. Health Psychol Behav Med. 2022;10(1):524-550.
- Seiler A, Camilo M, Korostovtseva L, et al. The importance of sleep for successful neurorehabilitation after stroke. Front Neurol. 2024;14:1322388.
- Fulk GD, Boyne P, Hauger M, et al. The impact of sleep disorders on functional recovery and participation following stroke: A systematic review and meta-analysis. Neurorehabil Neural Repair. 2020;34(11):1050-1061.
- Duss SB, Seiler A, Schmidt MH, et al. The role of sleep in recovery following ischemic stroke: A review of human and animal data. Neurobiol Sleep Circadian Rhythms. 2017;2:94-105.
- Webb AJS, Fonseca AC, Berge E, et al. Value of treatment by comprehensive stroke services for the reduction of critical gaps in acute stroke care in Europe. Eur J Neurol. 2021;28(2):717-725.
- Freburger JK, Cummings DM, Duncan PW, et al. The cost of implementing and sustaining the COMprehensive post-acute stroke services model. J Am Geriatr Soc. 2021;69(2):427-434.
- Mei YX, Xiang MQ, Zhang YM, et al. Economic evaluation of an enhanced post-discharge home-based care program for stroke survivors. J Adv Nurs. 2024;80(6):2482-2492.
- Parreiras MM, Gama GMDGN, Nascimento LR, et al. Stroke rehabilitation pathways during the first year: A cost-effectiveness analysis from a cohort of 460 individuals. NeuroRehabilitation. 2024;54(3):463-476.
Useful Resources
- CDC Stroke Prevention Guidelines – Comprehensive resources for primary and secondary stroke prevention, including evidence-based recommendations for lifestyle modification.
- WHO Physical Activity Recommendations – Global guidelines on physical activity levels for health, applicable to stroke recovery populations.
- American Stroke Association Recovery Resources – Patient and caregiver resources for understanding stroke recovery, rehabilitation options, and lifestyle changes.
- NICE Stroke Rehabilitation Guidelines – Evidence-based clinical guidelines for stroke rehabilitation in adults, including intensity recommendations and multidisciplinary approaches.
Frequently Asked Questions
What is the difference between physical inactivity and sedentary behavior?
Physical inactivity means not meeting recommended physical activity guidelines (typically 150 minutes of moderate activity per week), while sedentary behavior refers to sitting or reclining activities with very low energy expenditure (≤1.5 METs). A person can meet exercise guidelines but still be highly sedentary if they sit for most of the day. Both need to be addressed separately in stroke recovery programs, as reducing sitting time provides health benefits independent of exercise levels.
Which behavior change model is best for stroke recovery programs?
No single model is “best”—the most effective programs often integrate elements from multiple frameworks. The Health Belief Model helps address motivation, the Theory of Planned Behavior incorporates social support, and Social Cognitive Theory recognizes environmental factors. Research shows that combined model interventions improve outcomes more than single-framework approaches.
What does a multi-domain intervention include?
A comprehensive multi-domain intervention addresses the full 24-hour movement spectrum: structured exercise (aerobic and resistance training), incidental physical activity (movement throughout the day), sedentary behavior reduction (breaking up prolonged sitting), and sleep optimization. It should also include behavior change support like goal-setting, self-monitoring, and problem-solving strategies tailored to individual needs.
How much do comprehensive stroke recovery programs cost compared to traditional approaches?
While comprehensive programs have higher upfront costs, they demonstrate superior cost-effectiveness. Full implementation of comprehensive stroke services costs approximately $6,900 per quality-adjusted life year gained, well below standard cost-effectiveness thresholds. Models like COMPASS, with annual implementation costs around $75,000, can achieve net cost savings by preventing just six hospital readmissions per year (each costing ~$14,200).
How can comprehensive programs be implemented in existing healthcare systems?
Successful implementation requires several key elements: training healthcare professionals in behavior change techniques and multi-domain assessment, using intervention mapping frameworks to systematically develop programs, starting with transitional care models that bridge hospital to home, leveraging telehealth and digital tools to extend reach, and building partnerships with community organizations to provide accessible options. The Paul Coverdell National Acute Stroke Program offers a model for state-level coordination.
Future Blog Topics
| Upcoming Article | Coming Soon | Why It Matters |
|---|---|---|
| Sleep Architecture Changes After Stroke: What Policymakers Need to Know | Next Month | Deep dive into how stroke alters sleep patterns and why sleep optimization should be a mandatory component of recovery programs |
| Breaking Down Sedentary Behavior: Evidence-Based Interventions for Stroke Survivors | 6 Weeks | Practical strategies for reducing sitting time in stroke survivors, with implementation guidelines for rehabilitation facilities |
| Incidental Physical Activity: The Hidden Recovery Tool Policymakers Overlook | 2 Months | Why activities of daily living and light movement throughout the day may be as important as structured exercise for long-term outcomes |

Leave a Reply